Percutaneous Nephrolithotomy (PCNL) FAQs
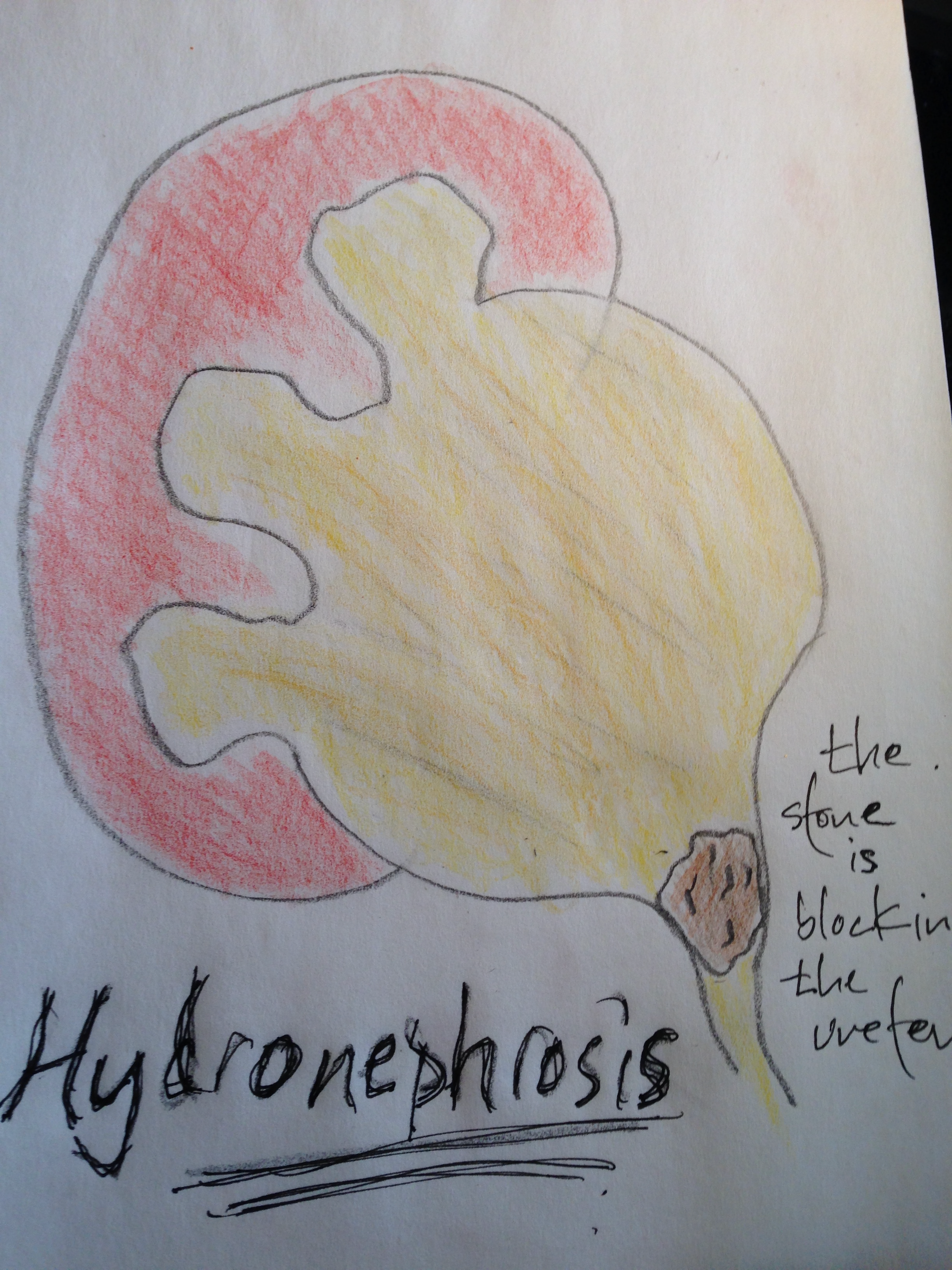
What is the diagnosis or pathology being treated by this procedure or surgery?
1
The diagnosis is a ureteral or kidney stone, obstructing or non-obstructing. For a percutaneous approach to be necessary the stone is often much larger making ureteroscopy more difficult.
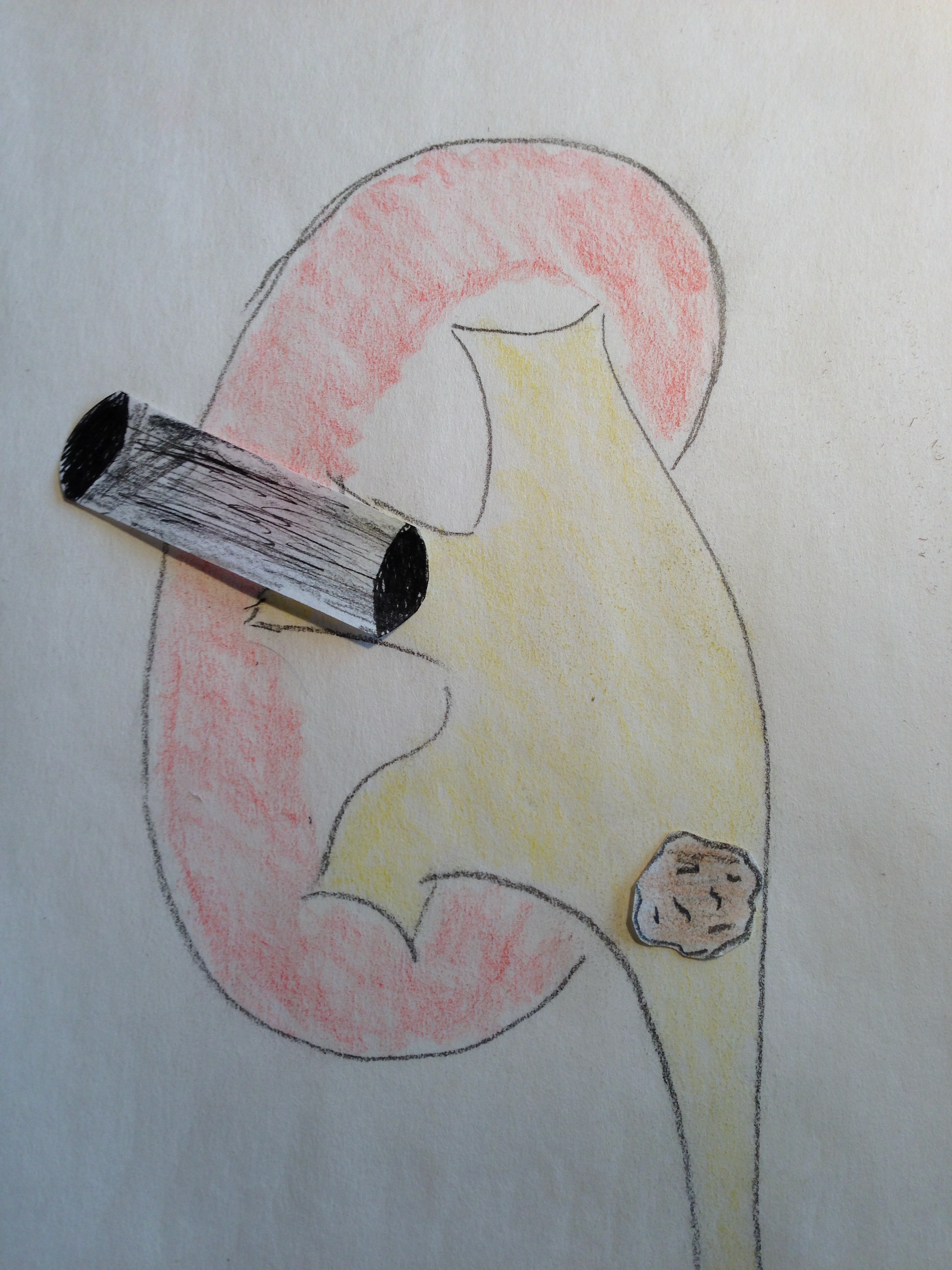
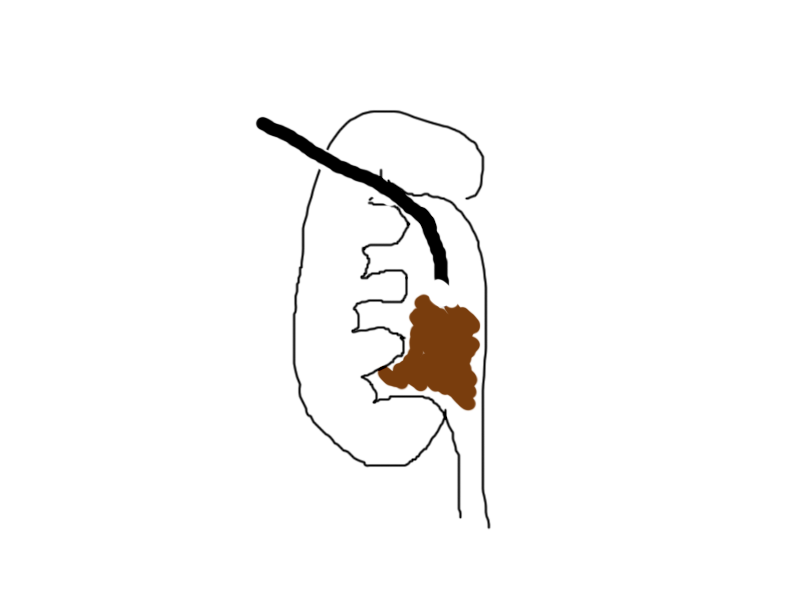
Can you describe the procedure or draw a picture?
2
Under general anesthesia a nephroscope is passed through a patient’s back and directly into the kidney. The direct access allows a larger scope to be passed. The stone is broken up using and ultrasonic, pneumatic, or laser lithotripter (sometimes all three). The large pieces are brought out through the access sheath.
This procedure is done in conjunction with an interventional radiologist in many cases who will help gain access to the kidney through the back.
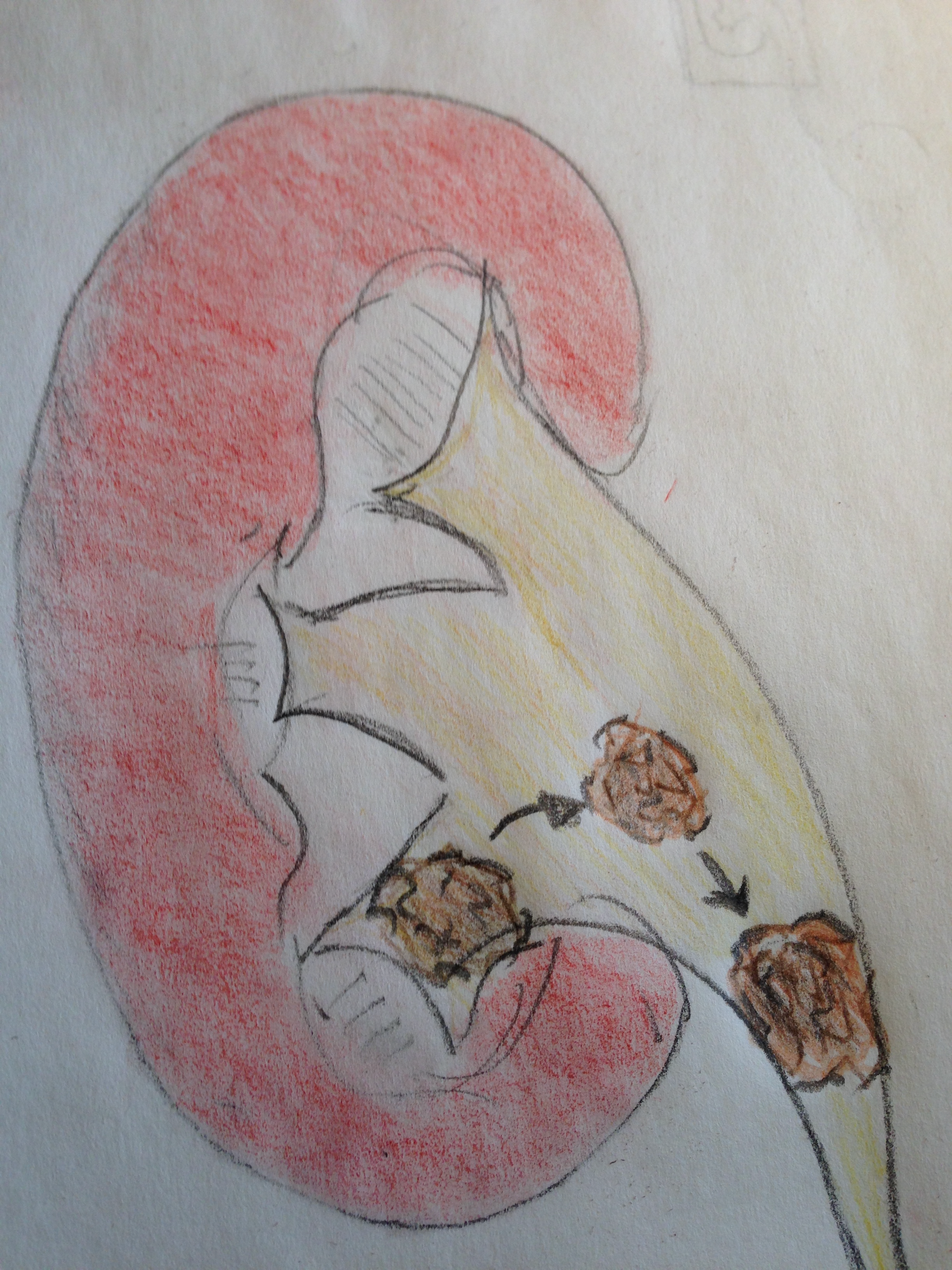
What are the benefits of doing this procedure?
3
The goal of doing this procedure is to render a patient stone-free. The benefit of doing this approach over other options is more stone can be removed
What are the risks of doing the procedure?
4
Bleeding: Bleeding is common and expected. The blood in the urine looks far worse than it is. Transfusion rates are rare. Delayed bleeding even a couple of weeks later is a possibility with this procedure.
Infection: This is a procedure with a high infection risk due to the foreign body (stent) and the obstruction of urine which causes stasis and risk of bacterial growth.
Failure to remove the stone: Stones are hard and the ureter is soft and delicate. There are plenty of times where the stone can’t be removed or be removed entirely with one procedure.
Injury to the kidney and ureter: A Nephrolithotomy should be performed erring always on safety and avoiding injury to the ureter and renal pelvis. Injuries are uncommon.
Anesthetic Risk: The risk of anesthesia is dependent on a patient’s age, health status and clinic condition.
Need for repeat procedure: Because of the nature of the procedure repeat procedures are necessary for some patients.
Pneumothorax/Hemothorax: The kidneys sits at the same level as the base of the diaphragm and chest cavity. Injury to the chest cavity can occur resulting in collapsed lung or blood and/or urine collections developing within the chest. This is uncommon.
Alternative procedures include Shock Wave Lithotripsy and ureteroscopy.
Are there alternatives to this procedure I should be considering?
5
Is this a common procedure?
6
Yes, this procedure is done nearly every day for obstructing kidney stones.
Should I do the procedure now or what happens if I wait to do the procedure?
7
Most obstructing stones need treatment emergently, urgently or semi-rugently to make sure the kidney is draining. The Percutaneous Nephroltihotomy is done electivelywhen a patient is stable, infection free.
How do I prepare for this surgery?
8
Standard precaution exist for most patients including pre-operative evaluation, diet restriction and avoidance of blood thinning medication.
How do I recover from this procedure?
9
The procedure is done with an overnight hospitalization. Most patients will have t a ureteral stent but some patients will need a nephrostomy tube left in place draining through the back after the procedure. The stent causes bleeding, infection risk, some discomfort. Patients with good pain control can resume normal activity within a few days. The stent will usually be removed 1-2 weeks the procedure. For patients who need repeat procedures the stent may remain in place until that procedure is performed.
Is this procedure covered by insurance?
10
Yes, this is covered by insurance.